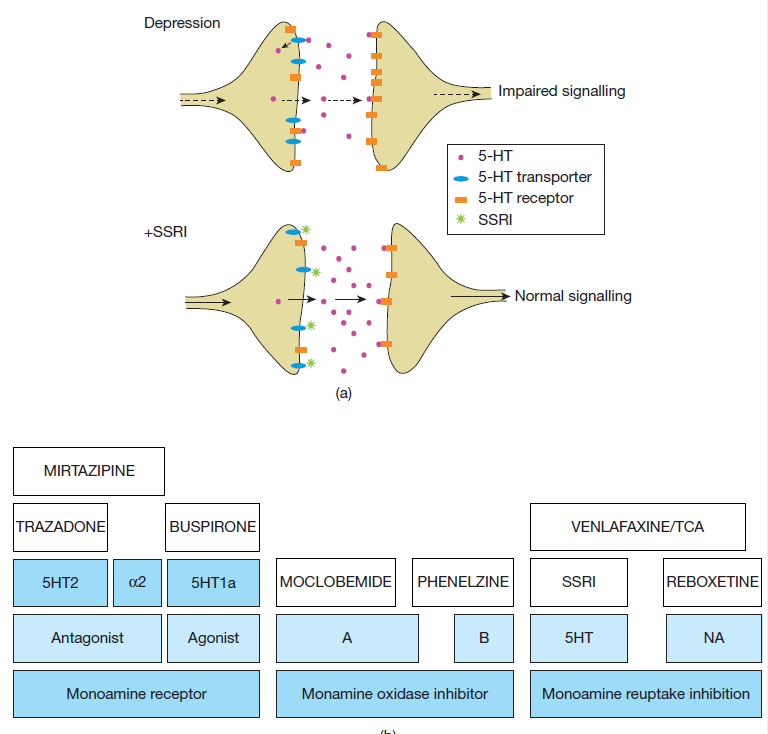
(a) A highly simplified schema for the proposed mechanism of action of selective serotonin reuptake
inhibitors (SSRIs). In depression, there is thought to be a relative 5-HT deficiency, and upregulation of 5-HT receptors.
The net effect is abnormal signalling and functioning of the postsynaptic neuron. SSRIs block the 5-HT transporter,
and increase 5-HT in the synapse. The antidepressant effect takes several days to occur, because other adaptive
changes also have to occur (to restore normal fi ring of the neuron, downregulate receptors, and other secondary
effects). Tricyclic antidepressants (TCAs) work similarly, but act upon presynaptic receptors and noradrenergic
synapses too. (b) An aide-memoire for the mechanism of action of various antidepressants. The receptors on which
the antidepressants work often also give an indication of what side effects to expect.
[Antidepressants]
Antidepressants are effective, readily available and a first-line treatment for depressive disorders. Some are also used to treat other disorders such as obsessivecompulsive disorder (OCD). The major classes are shown in Table 7.1. Selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs) have similar efficacy, with about 60% of patients responding after 6 weeks. Over the same period, 30–40% respond to placebo. Patients often want to stop antidepressants too soon.
Antidepressants usually produce some reduction in symptoms by 4–6 weeks, but it may take many months for the patient to recover fully. Continued treatment maintains the improvement in the medium term (6–9 months after getting better). Prolonged use halves the chances of relapse in those at risk.
[Selective serotonin reuptake inhibitors (SSRIs)]
SSRIs are the usual fi rst-line antidepressant.
• Mode of action.
Selectively inhibit synaptic 5-HT reuptake transporters, thereby increasing synaptic 5-HT concentration (Figure 7.1a).Practical usage. Start at full dosage, once daily with breakfast. Onset of antidepressant action becomes evident in 7–14 days. However, side eff ects (see below) occur in the fi rst few days – remember to warn the patient of this. Consider giving a hypnotic for the fi rst few weeks to aid sleep. Always withdraw an SSRI slowly at the end of treatment.
• Individual SSRIs.
There are some modest differences in properties between SSRIs. A good first choice is sertraline (50–100 mg/day),
which is effective, well tolerated, has few interactions with other drugs, and maybe is associated with a lower
incidence of sexual dysfunction. Escitalopram (10 mg/day) is also well tolerated although not available generically and therefore more expensive.
Fluoxetine (20–40 mg/day) has a long halflife, so is useful if compliance is poor, and withdrawal reactions are rare (but drug interactions persist longer).
• Side effects.
Usually well tolerated, though 15% have nausea, abdominal discomfort, diarrhoea, insomnia and agitation, mainly in the early stages. Sexual dysfunction (lack of libido, anorgasmia) is common in women and also occurs in men. SSRIs may increase the risk of upper gastrointestinal, bleeding and hyponatraemia. Some people experience discontinuation symptoms (insomnia, nausea, dizziness, agitation) when stopping the drug; hence withdraw over a few weeks.
• SSRIs and suicide.
There have been concerns that SSRIs are associated with an increase in suicidal thoughts and behaviour in the early stages of treatment, particularly in younger adults and children. Patients should always be monitored for suicide risk carefully at this time. However, this must be set against the reduction in suicide risk associated with the effective treatment of depression.
• Overdose.
Few effects; rarely if ever fatal. Citalopram is significantly more toxic in overdose than other SSRIs.
• Cautions and contraindications.
Few.
May increase seizures in epilepsy.
Coadministration with serotonergic drugs (including monoamine oxidase inhibitors (MAOIs),
l-tryptophan, lithium and St John’s wort) may lead to serotonin syndrome, a potentially lifethreatening condition that includes tachycardia, shivering, sweating, hyperthermia and hyperreflexia, progressing to shock and renal failure.
[Selective serotonin and noradrenaline reuptake inhibitors(SNRIs)]
Venlafaxine (75–375 mg/day) and duloxetine(60 mg/day) are the only members of this group.
• Mode of action.
SNRIs potently block 5-HT and NAreuptake but do not block cholinergic receptors.
• Practical usage.
Venlafaxine (but not duloxetine) is slightly more eff ective than SSRIs. Its main indication is for SSRI non-response. Give twice daily, though a long-acting (once daily) form is available.
• Side effects.
Resemble those of SSRIs, but maybe worse.
At high doses, hypertension may occurand should be monitored. Not sedative. Avoid MAOIs.
[Noradrenaline and serotonin specifi c antidepressant (NASSA)]
Mirtazapine (15–45 mg nocte).
• Mode of action.
Increases activity in the NA and 5-HT systems by blocking the negative feedback of NA on presynaptic alpha-2 receptors. Alpha-2
blockade also enhances 5-HT release.
• Practical usage.
Often used as a second-line treatment, and in combination with SSRIs as a thirdline treatment.
• Side effects.
Relatively sedating although this is not dose dependent. Less sexual dysfunction or nausea than SSRIs. Associated with weight gain.
'Psychiatry' 카테고리의 다른 글
| 의학통계-기초(1) (0) | 2022.11.26 |
|---|---|
| BENZODIAZEPINE EQUIVALENCE TABLE (0) | 2022.10.09 |
| 10 point guide to MSE in PSYCHIATRY (23) | 2022.03.07 |
| [재인용] 양극성장애 관련 조직, 웹사이트, 간행물 (0) | 2020.01.19 |
| 성인 주의력 결핍 과잉행동장애(Adult attention-deficit hyperactivity disorder) (0) | 2019.12.22 |